Pregnancy Care
Pregnancy Care

Breech Births
We will discuss and offer:
Simple exercises that are safe to do and may encourage your baby to move to a head-down position. The staff in the clinic will support you and we do not recommend you to perform these for the first time without support and guidance. These can be performed from 32 weeks onward.
- ECV Performed from 36-37 weeks
- Elective Caesarean Birth if the baby remains in Breech position
- Physiological vaginal Breech birth
What does ECV involve?
ECV involves applying gentle but firm pressure to your abdomen to help your baby turn in the uterus to lie head-first, Relaxing the muscles in your uterus with medication has been shown to improve the chances of turning your baby. This medication is given by injection before the ECV and is safe for both you and your baby, It may make you feel flushed and you may become aware of your heart beating faster than usual but this will only be for a short time. Before the ECV you will have an ultrasound scan to confirm if your baby is in breech position, and your pulse and blood pressure will be checked. After the ECV, the ultrasound scan will be repeated to see whether your baby has turned. Your baby’s heart rate will also be monitored before and after the procedure. You will be advised to contact the hospital if you have any bleeding, abdominal pain, contractions or reduced fetal movements after ECV.
ECV is usually performed after 36 or 37 weeks of pregnancy. However, it can be performed right up until the early stages of labour. You do not need to make any preparations for your ECV.
ECV can be uncomfortable and occasionally painful but your healthcare professional will stop if you are experiencing pain and the procedure will only last for a few minutes. If your healthcare professional is unsuccessful at their first attempt in turning your baby, then with your consent, they may try again. on another day. (If your blood type is Rhesus D negative, you will be advised to have an anti-Dinjection after the ECV and to have a blood test.)
Why turn my baby head-first?
If your ECV is successful and your baby is turned into the head-first position you are more likely to have a vaginal birth. A successful ECV lowers your chances of requiring a caesarean section and its associated risk.
Is ECV safe for me and my baby?
ECV is generally safe with a very low complication rate. Overall, there does not appear to be an increased risk to your baby from having ECV. After ECV has been performed, you will normally be able to go home on the same day. When you go into labour, your chances of needing an emergency caesarean section, forceps or vacuum (suction cup) birth is slightly higher than if your baby had always been in a head-down position. Immediately after ECV, there is a 1 in 200 chance of you needing an emergency caesarean section because of bleeding from the placenta and/or changes in your baby’s heartbeat.
ECV should be carried out by a doctor or a midwife trained in ECV. It should be carried out in a hospital where you can have an emergency caesarean section if needed. ECV can be carried out on most women, even if they have had one caesarean section before.
ECV should not be carried out if
- You need a caesarean section for other reasons, such as placenta praevia
- Your baby's heart rate tracing (also known as CTC) is abnormal.
- Your waters have broken
- You are pregnant with more than one baby
Is ECV always successful?
ECV is successful in about 50% of the cases. It is more likely to work if you have had a vaginal birth before. Your healthcare team should give you information about the chances of your baby turning based on their assessment of your pregnancy. If your baby does not turn then your healthcare professional will discuss your options for birth (see below), It is possible to have another attempt at ECV on a different day. If ECV is successful, there is still a small chance that your baby will turn back to the breech position. However, this happens to less than 5 in 100 (5%) women who have had a successful ECV
What are my options if my baby remains in breech position?
- Planned caesarean section
- Planned vaginal breech birth
- Your baby is in a certain position, for example, if its neck is very tilted back (hyperextended)
- You have a low-lying placenta (placenta praevia)
- You have preeclampsia or any other pregnancy problems
For more information, please attend the specialist Breech clinic where you will be able to have an individualised in-depth discussion with the team.
Speak to your obstetrician or your professional midwife to make an appointment with the breech specialist team, available across all the units of Fernandez Hospital. We can then discuss your options and make an individualised plan to support you.
Caesarean section
If your baby remains in breech position towards the end of the pregnancy, you should be given the option of a caesarean section. Research has shown that planned caesarean section is safer for your baby than a vaginal breech birth. The caesarean section carries slightly more risk for you than a vaginal birth. Caesarean section can increase your chances of problems in future. pregnancies. These may include placental problems, difficulty with repeat caesarean section surgery and a small increase in stillbirth in 5 subsequent pregnancies. If you choose to have a caesarean section but then go into labour before your planned operation, your healthcare professional will examine you to assess whether it is safe to go ahead. If the baby is close to being born, it may be safer for you to have a vaginal breech birth.
Footling breech (Incomplete breech)
When one or both feet of the baby are below its bottom.
Why are some babies breech?
Sometimes it is just a matter of chance that a baby does not turn and remains in the breech position. There are certain factors that make it more difficult for a baby to turn during pregnancy and therefore more likely to stay in the breech position.
- If this is your first pregnancy
- If your placenta is in a low-lying position
- (also known as placenta praevia)
- If you have too much or too little fluid
- (amniotic fluid) around your baby
- If you are having more than one baby
Very rarely, breech may be a sign of a problem with the baby. If this is the case, such problems may be picked up during the scan you are offered at around 20 weeks of pregnancy.
Vaginal birth
After discussion with your healthcare professional about you and your baby’s suitability for a breech delivery, you may choose to have a vaginal breech birth. If you choose this option, you will need to be cared for by a team trained in. helping women have breech babies vaginally. You should plan a hospital birth where you can have an emergency caesarean section if needed, as 4 in 10 (40%) women planning a vaginal breech birth do need a caesarean section. Induction of labour is not usually recommended. While a successful vaginal birth carries the least risks for you, it carries a small increased risk of your baby dying around the time of delivery. A vaginal breech birth may also cause serious short-term complications for your baby. However, these complications do not seem to have any long-term effects on your baby. Your individual risks should be discussed with you by your healthcare team. Before choosing a vaginal breech birth, it is advised that you and your baby are assessed by your healthcare professional.
They may advise against a vaginal birth if
- Your baby is a footling breech (one or both of the baby's feet are below its bottom)
- Your baby is larger or smaller than average (your healthcare team will discuss this with you)
- What if my baby is in breech position towards the end of my pregnancy?
- If your baby is suspected to be in breech position at 32-34 weeks, your
- Midwife or Obstetrician will refer you to the Breech specialist clinic at the location where you have been receiving care.
- At this clinic, you will be seen by our Breech specialist team who will discuss the options with you and your family.
- Breech baby at the end of pregnancy
This is useful for you if your baby remains in the breech position around. 34 weeks of pregnancy. Babies lying bottom first or feet first in the uterus (womb) instead of the usual head-first position is called breech babies. Breech is very common in early pregnancy, and by 36-37 weeks of pregnancy, most babies turn naturally into the head-first position. Towards the end of pregnancy, only 3-4 of every 100 (3-4%) babies are in the breech position.
Key points:
If your baby remains in the breech position, it does not mean that you or your baby have any problems.
A safer option is to put your baby in the head-first position so that you can have a vaginal delivery.
The alternative to turning your baby into the head-first position is to have a planned caesarean section or planned vaginal breech birth.
A breech baby may be lying in one of the following positions:
Frank breech
The baby is in the bottom first position with the thighs against its chest and feet up by its ears. Most breech babies are in this position.
Complete breech
The baby is in a bottom first position with its feet right next to its bottom. The thighs are against its chest and the knees are bent.
Pain Relief
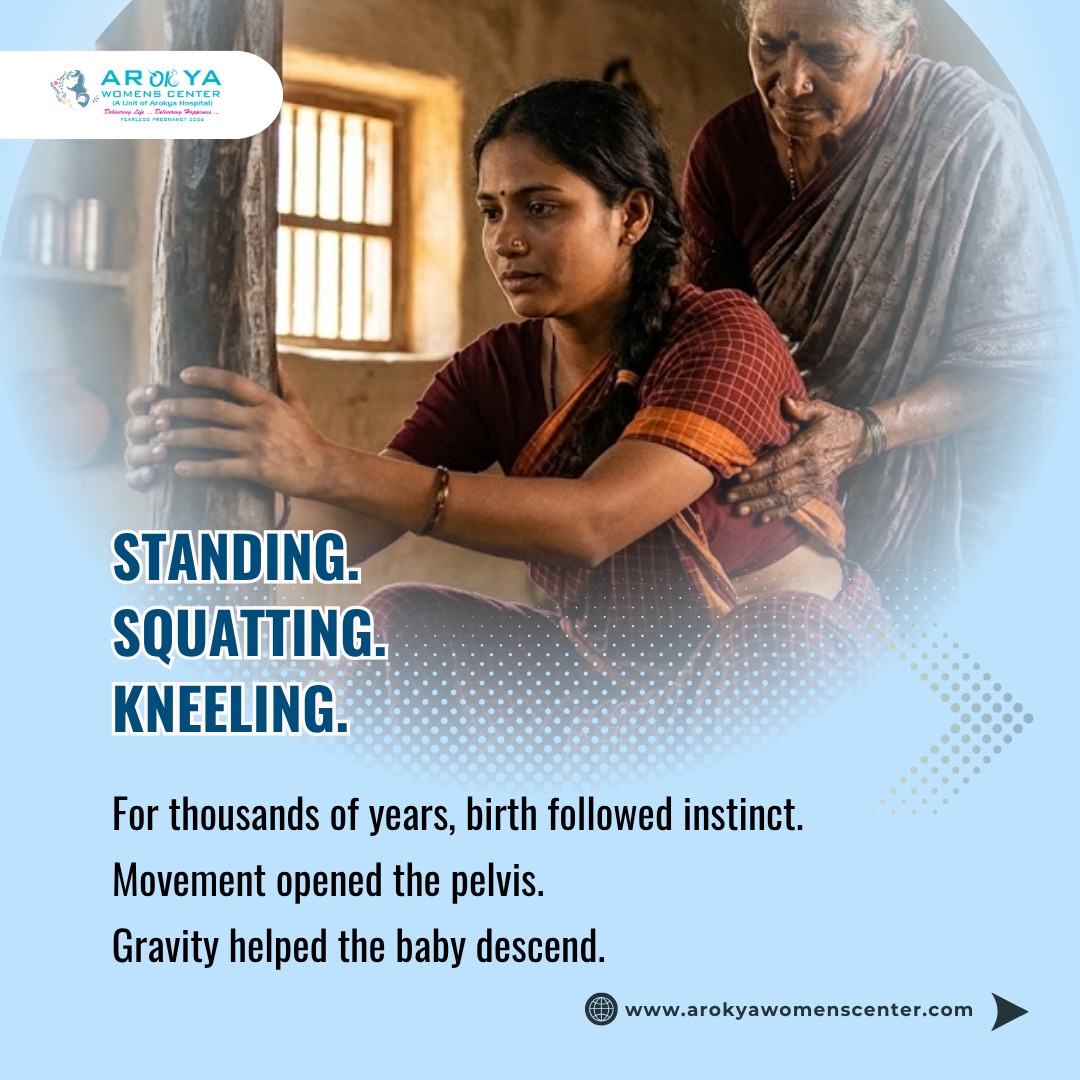
Natural Pain Relief Options
MASSAGE
Having someone rub your back will warm your skin and stimulate your body to release its own natural painkillers. A massage may help you to keep calm and cope with labour pain. Tell your birth partner or health professional where you’d like to be massaged. You may prefer it at the very base of your back during contractions. Or you may like your shoulders massaged between contractions to help you relax. Light skin stroking can stimulate oxytocin and also helps with relaxation and calmness.
NOTES
BREATHING TECHNIQUE
Focusing on your breathing is really a helpful way of getting through each contraction. Breathing in through your nose and breathing out through your mouth, keeping your mouth soft and slightly open is the right technique. Your health professional will explain and help once the contractions get stronger. When the contraction is over, try to relax as much as possible.
HYDROTHERAPY/WARM BATH
This can relax you and make contractions more bearable. It also helps to ease tummy ache or backache. Using a birth pool is likely to shorten the first stage of your labour and help you cope with the pain. Research has found that women who spend some time labouring in water are less likely to need any other form of pain relief when compared to women who spend their entire labour out of water.